A powerful cyclone roaring in the Arabian Sea was moving toward India’s western coast on Monday as authorities tried to evacuate hundreds of thousands of people and suspended COVID-19 vaccinations in one state.
Cyclone Tauktae, which has already killed six people in parts of southern India, is expected to make landfall on Monday evening in Gujarat state with winds of up to 175 kph (109 mph), a statement by the India Meteorological Department said.
After the cyclone slams ashore, forecasters warn of the potential for extensive damage from high winds, heavy rainfall and flooding in low-lying areas.
The massive storm comes as India is battling with a devastating coronavirus surge—and both the storm and the virus could exacerbate the effects of the other. The storm has already led to the suspension of some vaccination efforts and there is greater risk of virus transmission in crowded evacuation shelters
Virus lockdown measures, meanwhile, could slow relief work after the storm, and damage from the storm could potentially destroy roads and cut vital supply lines for things like vaccines and medical supplies needed for virus patients.
In Gujarat, vaccinations were suspended for two days and authorities worked to evacuate hundreds of thousands of people to temporary relief shelters. The state’s Chief Minister Vijay Rupani Monday asked officials to ensure that the oxygen supplies to hospitals are not disrupted.
In Maharashtra, operations at Mumbai city’s Chhatrapati Shivaji Maharaj International Airport were suspended for three hours.
Already, thousands of rescue and relief teams from the army, navy and coast guard, along with ships and aircraft, have been deployed for recovery operations.
India’s western coast no stranger to devastating cyclones, but changing climate patterns have caused them to become more intense, rather than more frequent.
In May 2020, nearly 100 people died after Cyclone Amphan, the most powerful storm to hit eastern India in more than a decade, ravaged the region and left millions without power.
With a relatively minor genetic change, a new treatment developed by researchers at the Georgia Institute of Technology and Emory University appears to stop replication of both flu viruses and the virus that causes COVID-19. Best of all, the treatment could be delivered to the lungs via a nebulizer, making it easy for patients to administer themselves at home.
The therapy is based on a type of CRISPR, which normally allows researchers to target and edit specific portions of the genetic code, to target RNA molecules. In this case, the team used mRNA technology to code for a protein called Cas13a that destroys parts of the RNA genetic code that viruses use to replicate in cells in the lungs. It was developed by researchers in Philip Santangelo’s lab in the Wallace H. Coulter Department of Biomedical Engineering.
“In our drug, the only thing you have to change to go from one virus to another is the guide strand—we only have to change one sequence of RNA. That’s it,” Santangelo said. “We went from flu to SARS-CoV-2, the virus that causes COVID-19. They’re incredibly different viruses. And we were able to do that very, very rapidly by just changing a guide.”
The guide strand is a map that basically tells the Cas13a protein where to attach to the viruses’ RNA and begin to destroy it. Working with collaborators at the University of Georgia, Georgia State University, and Kennesaw State University, Santangelo’s team tested its approach against flu in mice and SARS-CoV-2 in hamsters. In both cases, the sick animals recovered.
Their results are reported Feb. 3 in the journal Nature Biotechnology. It’s the first study to show mRNA can be used to express the Cas13a protein and get it to work directly in lung tissue rather than in cells in a dish. It’s also the first to demonstrate the Cas13a protein is effective at stopping replication of SARS-CoV-2.
What’s more, the team’s approach has the potential to work against 99% of flu strains that have circulated over the last century. It also appears it would be effective against the new highly contagious variants of the coronavirus that have begun to circulate.
The key to that broad effectiveness is the sequence of genes the researchers target.
“In flu, we’re attacking the polymerase genes. Those are the enzymes that allow the virus to make more RNA and to replicate,” said Santangelo, the study’s corresponding author.
With help from a collaborator at the Centers for Disease Control and Prevention, they looked at the genetic sequences of prevalent flu strains over the last 100 years and found regions of RNA that are unchanged across nearly all of them.
“We went after those, because they’re far better conserved,” Santangelo said. “We let the biology dictate what our targets would be.”
Likewise, in SARS-CoV-2, the sequences the researchers targeted so far remain unchanged in the new variants.
The approach means the treatment is flexible and adaptable as new viruses emerge, said Daryll Vanover, a research scientist in Santangelo’s lab and the paper’s second author.
“One of the first things that society and the CDC is going to get when a pandemic emerges is the genetic sequence. It’s one of the first tools that the CDC and the surveillance teams are going to use to identify what kind of virus this is and to begin tracking it,” Vanover said. “Once the CDC publishes those sequences—that’s all we need. We can immediately screen across the regions that we’re interested in to target it and knock down the virus.”
Vanover said that can result in lead candidates for clinical trials in a matter of weeks—which is about how long it took them to scan the sequences, design their guide strands, and be ready for testing in this study.
“It’s really quite plug-and-play,” Santangelo said. “If you’re talking about small tweaks versus large tweaks, it’s a big bonus in terms of time. And in pandemics—if we had had a vaccine in a month or two after the pandemic hit, think about what things would look like now. If we had a therapy a month after it hit, what would things look like now? It could make a huge difference, the impact on the economy, the impact on people.”
The project was funded by the Defense Advanced Research Projects Agency’s (DARPA) PReemptive Expression of Protective Alleles and Response Elements (PREPARE) program, with the goal of creating safe, effective, transient, and reversible gene modulators as medical countermeasures that could be adapted and delivered rapidly. That’s why the team decided to try a nebulizer for delivering the treatment, Santangelo said.
“If you’re really trying to think of something that’s going to be a treatment that someone can actually give themselves in their own house, the nebulizer we used is not terribly different from one that you can go buy at a pharmacy,” he said.
The team’s approach also was sped along by their previous work on delivering mRNA to mucosal surfaces like those in the lungs. They knew there was a good chance they could tackle respiratory infections with that approach. They decided to use mRNA to code for the Cas13a protein because it’s an inherently safe technique.
“The mRNA is transient. It doesn’t get into the nucleus, doesn’t affect your DNA,” Santangelo said, “and for these CRISPR proteins, you really don’t want them expressed for long periods of time.”
He and Vanover said additional work remains—especially understanding more about the specific mechanisms that make the treatment effective. It has produced no side effects in the animal models, but they want to take a deeper look at safety as they consider moving closer to a therapy for human patients.
“This project really gave us the opportunity to push our limits in the lab in terms of techniques, in terms of new strategy,” said Chiara Zurla, the team’s project manager and a co-author on the paper. “Especially with the pandemic, we feel an obligation to do as much as we can as well as we can. This first paper is a great example, but many will follow; we’ve done a lot of work, and we have a lot of promising results.”
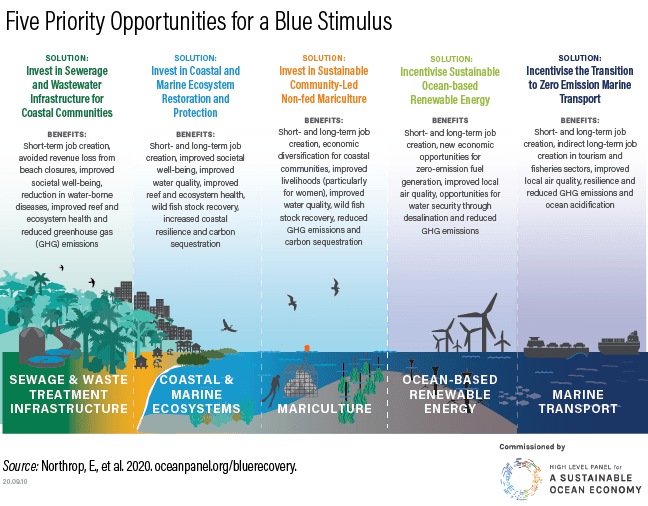
“The ocean economy may be a victim of the impacts of the COVID-19 crisis, but it also holds solutions for rebuilding a more resilient, sustainable and equitable post-COVID world.”
– A Sustainable & Equitable Blue Recovery to the COVID-19 Crisis Report
Ocean and coastal habitats provide an essential workplace for the world’s small-scale fishers, and coastal communities rely on the ocean for jobs, food, health, and cultural traditions. In fact, the ocean economy adds approximately US$1.5 trillion in value globally (OECD 2016). But the COVID-19 pandemic disproportionally impacts the ocean economy and these communities, especially those from Small Island Developing States (SIDS).
“A Sustainable and Equitable Blue Recovery to the COVID-19 Crisis”, as the name implies, recognizes the power of nature to help solve daunting global issues like climate change and pandemics. The report was released ahead of Climate Week NYC and a Rare-facilitated high-level roundtable meeting of coastal countries, where officials issued a joint message acknowledging the importance of the small-scale fishing sector to a blue (or green) recovery: that by implementing coastal and marine nature-based solutions, small-scale fishers can improve food security, nutrition, and the local economies of coastal nations, and enhance coastal resilience from climate change.
As a member of the Ocean Panel’s Advisory Network, Rare supports the five blue stimulus opportunities for government investment in COVID-19 crisis recovery outlined in the report. These proposed solutions deliver short-term relief to the economy and long-term economic, social, and environmental resilience. Moreover, they are considered a win-win for immediate assistance and forward-looking sustainable planning, known as a ‘no regrets’ investment strategy.
Fish Forever, Rare’s coastal fisheries program, prioritizes the report’s solution related to coastal and marine ecosystems: Invest in Coastal and Marine Ecosystem Restoration and Protection. Fish Forever uses behavioral insights to inspire fishing communities — fishers, fish buyers and traders, community members, and their local government — to adopt more responsible behaviors related to coastal fishing and implement nature-based solutions to protect their natural resources.
Investing in a nature-based solution like restoring and protecting coastal and marine ecosystems benefits coastal fishing households and their communities. This solution also has a host of benefits critical for a blue recovery, including the following five:
Improves Food Security – Protecting coastal ecosystems supports ample fish resources and fish breeding habitat, which safeguards fishing communities by strengthening food security during times of crisis. Technology innovations, like Rare’s OurFish App referenced in the report, show how a nature-based approach to resource management benefits the community and improves food security: the app digitally helps to manage and understand fish stock and finance trends and enables fishing communities to monitor the value, type and local amount of fish caught.
Enables Sound Financial and Household Decision-Making –Establishing Savings Clubs led by small-scale fishers empowers its members, often majority women, to manage their long-term household finances. It also raises awareness of the actions needed to enforce fish sanctuaries for coastal habitat protection and community livelihoods’ sustainability. This approach to behavior change “can powerfully affect the long-term strategy behind coastal fisheries conservation and the goal of ending overfishing,” as the report explains.
Enhances Economic, Social, and Environmental Resilience – Investing in coastal and marine ecosystem restoration and protection can also expand job opportunities, such as protected areas enforcement officers, development planners, environmental engineers, and ecological restoration scientists. In addition to job security, nature-based solutions support the healthy natural resources that protect small-scale fishers’ livelihoods.
Manages Natural Resources Sustainably – Ensuring coastal and marine ecosystem integrity further increases economic productivity by improving fisheries and tourism opportunities. Sustainable management also allows for more significant investment opportunities in blue carbon activities focused on climate mitigation and adaptation benefits from mangroves, seagrasses, and tidal salt marshes.
Builds Community Pride – Stakeholder engagement and collaboration with public and private sectors, including small-scale fishers and their families, are critical for building pride in and ownership of more sustainable behaviors and community-based programs. Co-owning and managing natural resources and ensuring the inclusion of women and Indigenous communities has also demonstrated long-lasting benefits and delivers on many of the UN’s sustainable development goals.
Farmers and fishers rely on healthy ecosystems and strong local governance and management to thrive. Building back better from the impacts of COVID-19 will require a global blue recovery effort that not only prioritizes nature-based solutions but empowers coastal communities and their leaders to champion blue solutions.
Massachusetts General Hospital pathologist James Stone can tell that most of the hearts he’s examined from COVID-19 patients are damaged from the first moment he holds them. They’re enlarged. They’re heavy. They’re uneven.
What he can’t tell—at least until he starts looking at samples of the tissue under a microscope—is exactly how those hearts were damaged, and whether it is a direct result of SARS-CoV-2 infection.
Early in the pandemic, other clinicians noted that even some patients who didn’t have preexisting heart conditions experienced cardiovascular damage while fighting COVID-19 infections, pointing to a possible causative link. Researchers had found, for example, that 8–12 percent of hospitalized COVID-19 patients had elevated levels of muscle contraction–regulating proteins called troponins—a sign of heart damage—and that these patients had an increased risk of mortality compared with those who didn’t have excess troponins. And early observations of patients in China who suffered reduced ejection fraction—the amount of blood getting pumped out of the heart each time it contracts—led researchers to suggest that these individuals were likely experiencing myocarditis, a severe form of inflammation that can weaken the heart and is commonly associated with infections.
But Stone and his collaborators’ analysis of heart tissue from 21 patients who died of COVID-19, published today (September 24) in the European Heart Journal, shows that while 86 percent of the patients did have inflammation in their hearts, only three had myocarditis. Several had other forms of heart injury, such as right ventricular strain injuries.
“The problem we identified in this study is that there’s other types of myocardial injury in these patients that is also causing elevated troponins,” says Stone. His international team sought to determine the mechanisms through which the disease damaged the heart and found that some conditions “really haven’t been talked about at all in the [COVID-19] papers that have previously been published.”
The pathologists observed a median of 20 slides from each heart, which is more than are included in most other studies regarding COVID-19’s cardiac effects. George Abela, a cardiologist at Michigan State University who was not involved in the study, tells The Scientist in an email, “This provides a more in-depth view of the extent of injury.”
The researchers expected to find some macrophages, a type of white blood cell that indicates inflammation, as pathologists had observed macrophages in the hearts of SARS patients during the 2003 outbreak. But Stone says he was surprised to see just how common these were—18 out of 21 COVID-19 patients’ hearts harbored macrophages that exhibited this type of inflammation. “It was really quite extensive,” he says.
As they analyzed the hearts further, the pathologists noted that only three patients had myocarditis, while four showed signs of heart injury due to right ventricular strain and another four had small blood clots in the vessels in the heart. It’s not clear why patients experience such inconsistent cardiac issues.
Abela says these findings have implications for treatment. For example, if the patient has right heart failure, a condition where the right side of a patient’s heart is not pumping enough blood to the lungs, a device that mechanically helps the heart pump blood might help, rather than drugs that target the inflammation or infection, which could be used to treat myocarditis.
Because so many of the hearts were infiltrated by macrophages, the researchers say that it may be difficult to discern who is experiencing myocarditis, which is characterized by different inflammatory cells—lymphocytes—while patients are alive. The two cell types would appear similar on tests that image the hearts of living patients. So, the team looked back at the patients’ medical records to see if they could find patterns in clinical tests that would reveal the type of heart damage when it still might be treatable. The three patients with myocarditis all had both troponin levels above 60 ng/mL and abnormal ECG readings while in the hospital. Only 15 percent of the patients without myocarditis had this combination.
The findings need to be replicated in larger groups of patients but could help doctors determine the best course of treatment for heart damage due to COVID-19, Stone says. The study is “giving the cardiologists and the ICU doctors that are taking care of these patients a roadmap of the changes that are going on in the heart.”
“Novel disease entities like SARS-CoV-2 reinforce the tremendous importance of continuing our efforts at continuing to facilitate autopsy evaluations,” says Allan Jaffe, a cardiologist at the Mayo Clinic, in an email. “This consortium of hospitals have added substantially to our knowledge of Covid disease.”
— Many individuals show subclinical abnormalities as well as differences from symptomatic patients
Asymptomatic individuals carrying SARS-CoV-2 shed the virus longer than those with COVID-19 symptoms, with other lab findings suggesting the symptomatic patients mounted more robust immune responses, a small study in China found.
Median duration of viral shedding among 37 asymptomatic patients was 19 days (interquartile range 15-26; range 6-45) versus 14 days among 37 matched symptomatic patients (IQR 9-22; log-rank P=0.028), reported Jing-Fu Qiu, PhD, of Chongqing Medical University, and colleagues, though viral shedding does not necessarily mean the patients were infectious.
Virus-specific IgG antibody titers and cytokine levels were also significantly lower among asymptomatic patients in the acute phase of infection, when viral RNA can be found in respiratory specimens, the authors wrote in Nature Medicine — both of which indicated that immune responses weren’t as strong in the asymptomatic group.
Asymptomatic transmission of COVID-19 is one of its biggest mysteries, with the World Health Organization recently reminding the public of the distinction between asymptomatic patients, who never develop symptoms, and presymptomatic patients, who go on to develop symptoms later in the course of disease.
Qiu and colleagues characterized asymptomatic carriers as the “silent spreaders” of COVID-19.
“However, our understanding of the clinical features and immune responses of asymptomatic individuals with SARS-CoV-2 infection is limited,” the researchers added.
For the study, they examined data from 178 patients with PCR-confirmed SARS-CoV-2 infection in the Wanzhou District in China, including 37 without symptoms. Median age in the latter was 41, and 22 were women. These individuals were matched by age, sex, and comorbidity with 37 symptomatic patients for antibody detection and cytokine measurement. Qiu and colleagues also included a group of 37 individuals who tested negative via RT-PCR for cytokine comparisons.
Lab values and imaging were not entirely normal for the asymptomatic group. Eleven had increased C-reactive protein levels and six had elevated levels of alanine aminotransferase. Chest CT found “focal ground-glass opacities” in 11 and “stripe shadows and/or diffuse consolidation” in another 10 of the group; in two-thirds of these 21 patients, the abnormalities were in only one lung. The remaining 16 showed entirely normal imaging.
Around 80% of both symptomatic and asymptomatic patients tested positive for IgG antibodies about 3-4 weeks after exposure. The difference was greater when examining IgM antibodies, with positive findings in 78.4% of symptomatic patients and 62.2% of asymptomatic patients.
In the early convalescent phase, defined as 8 weeks after hospital discharge, symptomatic patients had higher IgG levels, though both groups experienced over 90% decreases in IgG levels. A larger proportion of asymptomatic patients had decreases in neutralizing serum antibody levels versus symptomatic patients (81.1% vs 62.2%, respectively).
These findings should serve as a caution against assuming prior infection confers immunity to future infection, Qiu and colleagues said.
“These data might indicate the risks of using COVID-19 ‘immunity passports’ and support the prolongation of public health interventions, including social distancing, hygiene, isolation of high-risk groups, and widespread testing,” the team wrote.
Plasma levels of cytokines were also similar between asymptomatic patients and healthy controls, though significantly higher levels of stem cell factor and leukemia inhibitory factor were found in the asymptomatic group, the researchers noted, calling this a “reduced inflammatory response characterized by low circulating concentrations of cytokines and chemokines.”
Qiu and co-authors cited the varying sensitivity and specificity of antibody tests (obtained from a company called Bioscience) as a limitation to their study, adding that the results may be confounded by existing antibodies to other coronaviruses, such as SARS or MERS, as well as common cold viruses.
Coronaviruses were first identified as human respiratory pathogens, in the year 1965, and were known to demonstrate very high rate of mutation. Coronaviruses are enveloped (+) RNAs, that replicate in the cytoplasm. To deliver their nucleocaspid into the host cell, they rely on the fusion of their envelope with the host cell membrane. The spike glycoprotein (S) mediates this entry of the virus and acts as the primary determinant of cell tropism and pathogenesis. Glycoprotein (S) is classified as a class I fusion protein and is reponsible for binding to the receptor on the host cell, whilst mediating the fusion of the host and viral membranes. This is a process driven by major conformational changes of the S protein. On more technical terms, Corona viruses are the containers of the largest ssRNA genome of 33kb. Structurally, coronaviruses are enveloped viruses with round or pleomorphic virions which are 80 to 120 nm in diameter
This 1st generation of coronaviruses could not survive for long, owing to the host resistance. However, in 2002, new strains of these coronaviruses emerged. These strains of Coronaviruses had very similar genome sequences, and had been isolated from animals sold at markets, in China, where the first SARS cases had appeared. Antibodies to these viruses were found in people in China and some bat species. This small outbreak of corona can be consideed as one due to the 2nd generation of Corona viruses.
Finally, the Coronavirus outbreak of 2020-this outbreak had presented itself in the form of pneumonia of an unknown etiology, in Wuhan, China. This is named as SARS-CoV-2. It can be implied that recombination could have occurred, either by viral-viral or viral-host genes committing acts of “molecular piracy” to invade vertebrates and render them immunocompromised. This pandemic begets an extensive line of research by the world’s brightest to solve this enigma, consequently putting an end to it.
After the lockdown due to Covid-19 in many countries, there was lesser travelling done by people, whether by cars, trains or flights. Even many industries were non-functional. This led to the significant decrease in air pollution, as there was a marked reduction in nitrous oxide emission.
Lockdown has decreased the fishingactivity, hence the fish biomass will increase. Even the sea turtles have been spotted returning to areas they once avoided to lay their eggs, all due to the lack of human interference.
Plants are growing better because there is cleaner air and water, yet again there is no human interference.
Less litter means lesser clogging of river systems, which is good in the long run for the environment.
In conclusion, though there has been a positive impact on the environment due to the lockdown, there is a fear that once people start travelling, all these positive impacts will soon disappear.