Mumbai is the first city to report a case of omicron XE variant, In the U.K., the XE variant was discovered and is a mutation of B.1 and B.2 strains of Omicron. The WHO is currently tracking the XE mutation as part of the Omicron variant. Micron symptoms can include fever, sore throat, scratchy throat, cough and cold, skin irritation and discoloration, gastrointestinal distress, and a dry cough.
Omicron XE Variant
It was detected in the United Kingdom in January 2022 that the new variant XE of COVID-19 was identified. The WHO considers it ten times more contagious than the BA.2 variant. India’s COVID-19 XE variant has recently been updated
Once again, there has been an increase in the Coronavirus outbreak. There has been a fourth wave of Coronavirus in Asia and Europe during the past few weeks. There has been a sudden increase in new cases suspected to be caused by the corona subvariant omicron BA.2. Researchers have found a new corona XE variant in this hour of crisis.
Omicron XE Variant Symptoms
According to the organization, it is difficult to say whether it is fatal given the current situation, but knowing the signs and symptoms will help one avoid contracting the infection. Here are some symptoms of this new variant of the Coronavirus.
This variant is currently being studied. It is common for such a condition to cause early symptoms like fever, sore throat, cough, mucus and cold, and stomach problems. Additionally, the new variant can be even more dangerous for those already ill.
Since it is a mutation of the original Omicron, the vaccine may affect the new variant. The omicron effect in India was different from that in the second wave because of the large number of vaccinations during the third wave.
Omicron XE Variant Severity
Doctor Allison Arwady, Commissioner of Chicago’s Department of Public Health, said Tuesday that omicron “is likely to spread rapidly” and even more rapidly than the delta variant responsible for most of the latest outbreaks in the U.S.
It’s probably three times as contagious as the delta variant. Director Rochelle Walensky said Omicron has a two-day doubling time shorter than delta, indicating higher transmissibility. According to a study released Tuesday, the variant of the virus that is causing a surge in infections in South Africa is better at evading vaccines and causing less severe illness.
However, the data also shows that although the number of cases is increasing, hospitalizations are not rising as fast, which leads scientists to believe that the risk of hospitalization due to the virus is lower than that related to delta or earlier variants. A study adjusted for vaccination status found that admitted adults diagnosed with COVID-19 were 29% fewer than those diagnosed with the wave in mid-2020.
Omicron XE Variant Cases so Far
It is not the vaccine but reaching those at risk that has been the challenge.
Upon being asked if an Omicron vaccine was required, Mahamud said it was too early to tell but stated that a global approach should be taken and that manufacturers should not have the sole decision-making authority.
If you go ahead with Omicron, then a new antigen may emerge that is more immunoevasive or transmissible,” he said. A WHO technical group had recently met to discuss vaccine composition.
In his view, the most effective way to reduce the impact of this variant would be for the WHO to have 70% of each country’s population vaccinated by July, rather than offering third and fourth doses in some nations.
As the number of cases due to Omicron has risen, some countries, including the United States, have shortened quarantine periods for healthy people and allowed them to return to work or school earlier.
According to Mahamud, leaders should decide how strong the local epidemic is. Countries with high numbers of cases may need to omit isolation periods to maintain essential services.
Some places have shut mainly it out, so maintaining the entire 14-day quarantine period might be the best option. You should invest heavily in keeping your numbers very low if your numbers are tiny.
When an atomic or nuclear bomb detonates, the 1 megaton blast kills or poisons everything within a two-mile radius. The accident at the Chernobyl power plant in 1986 and the bombs dropped on Hiroshima and Nagasaki in 1945 provide insight into the short and long-term effects of radiation and thermonuclear detonation on the environment. If enough nuclear weapons were exploded in a large-scale nuclear war, vast areas of the earth would become uninhabitable.
Immediate Environmental Effects
When an atomic bomb explodes, plutonium in the device undergoes fission, releasing enormous quantities of energy. The initial blast creates a blinding flash, followed by temperatures in the area of the explosion reaching upwards of 10 million degrees Celsius. Electromagnetic radiation leads to the formation of a fireball. A crushing wind caused by the initial blast destroys buildings and trees in its path. A single 15 kiloton bomb detonated over the center of Hiroshima near the end of World War II, destroying everything within a 1-mile radius of the city. The effect on the immediate environment is one of total devastation. The extreme heat of thermal radiation burns everything in its path, including animals, trees, buildings and people. Many of those who did not die from radiation or burns later developed cancers from the radiation.
Explosive Fallout
The detonation of an atomic bomb creates radioactive dust that falls out of the sky into the area around the site of the explosion. Wind and water currents carry the dust across a much larger radius than the initial explosion, where it contaminates the ground, water supply and the food chain. Initially, little was known about radioactive fallout. In the 1950s, scientists in the United States discovered from nuclear weapons testing that the particles in this dust were comprised of split atoms that were highly radioactive and dangerous. Radioactive particles from nuclear fallout also can contaminate both wild and domesticated animals, as well as agricultural plants.
Radiation Effects
The release of radiation from the Chernobyl power plant gives scientists an idea of what the effects would be on the environment in a small nuclear war. The amount of radiation released at Chernobyl is equivalent to the detonation of about a dozen atomic bombs at an altitude that would cause maximum blast damage. At Chernobyl, large amounts of radioactive particles called iodine-131 and cesium 137 were released into the environment during a fire that burned for 10 days. These isotopes are particularly dangerous to living organisms.
Water and Forest Contamination
Radioactive particles can travel from the site of an atomic bomb explosion and contaminate bodies of water, including aquatic life like fish. In addition, the fallout from the detonation of numerous atomic bombs would result in the contamination of berries and other plant life found in the surrounding areas and forests. Genetic mutations and disease in the generations of animals and humans following contamination would also occur. Animals in Chernobyl’s forests, for example, have high levels of radioactive cesium. Scientists expect the contamination to remain that way for decades.
Having just yet won the war against covid, we are again glued to the screens of our TVs catching up the escalating war tensions between Russia and Ukraine. Of course, we hope that it doesn’t turn into a full-fledged war because the horrible effects of war on mankind are known to one and all. But today, let’s ponder on the effects of war on environment.
The natural environment has been a strategic element of war since the first rock was thrown by the first cave dweller. The armies of ancient Rome and Assyria, to ensure the total capitulation of their enemies, reportedly sowed salt into the cropland of their foes, making the soil useless for farming—an early use of military herbicide, and one of the most devastating environmental effects of war.
But history also provides lessons in eco-sensitive warfare. The Bible, in Deuteronomy 20:19, stays the hand of the warrior to minimize war’s impact on nature and men alike:
“When you besiege a city a long time, to make war against it in order to capture it, you shall not destroy its trees by swinging an axe against them; for you may eat from them, and you shall not cut them down. For is the tree of the field a man, that it should be besieged by you?”
War and the Environment: We’ve Been Lucky so Far
War is waged differently today, of course, and has widespread environmental impacts that last far longer. “The technology has changed, and the potential effects of the technology are very different,” says Carl Bruch, director of international programs at the Environmental Law Institute in Washington, D.C.
Bruch, who is also the co-author of “The Environmental Consequences of War: Legal, Economic, and Scientific Perspectives”, notes that modern chemical, biological, and nuclear warfare has the potential to wreak unprecedented environmental havoc that, fortunately, we haven’t seen—yet. “This is a great threat,” Bruch says.1
But in some cases, precision weapons and other technological advances can shield the environment by targeting key facilities, leaving other areas relatively unscathed.2 “You could make the argument that these weapons have the ability to minimize collateral damage,” says Geoffrey Dabelko, senior advisor to the Environmental Change and Security Program at the Woodrow Wilson Center for Scholars in Washington, D.C.
It’s Local: The Impact of War Today
Warfare today also occurs infrequently between independent nations; more often, armed conflict breaks out between rival factions within a nation. These localized civil wars, according to Bruch, are usually beyond the reach of international treaties and bodies of law. “Internal conflict is viewed as a matter of sovereignty—an internal matter,” he says. As a result, environmental damage, like human rights violations, occurs unchecked by outside organizations.
Though skirmishes, armed conflicts, and open warfare vary tremendously by region and by weapons used, the effects of war on the environment usually involve the following broad categories.
Habitat Destruction and Refugees
Perhaps the most famous example of habitat devastation occurred during the Vietnam War when U.S. forces sprayed herbicides like Agent Orange on the forests and mangrove swamps that provided cover to guerrilla soldiers. An estimated 20 million gallons of herbicide were used, decimating about 4.5 million acres in the countryside. Some regions are not expected to recover for several decades.
Invasive Species
Military ships, cargo airplanes, and trucks often carry more than soldiers and munitions; non-native plants and animals can also ride along, invading new areas and wiping out native species in the process. Laysan Island in the Pacific Ocean was once home to a number of rare plants and animals, but troop movements during and after World War II introduced rats that nearly wiped out the Laysan finch and the Laysan rail, as well as bringing in sandbur, an invasive plant that crowds out the native bunchgrass that local birds depend on for habitat.
Infrastructure Collapse
Among the first and most vulnerable targets of attack in a military campaign are the enemy’s roads, bridges, utilities, and other infrastructure.6 While these don’t form part of the natural environment, the destruction of wastewater treatment plants, for example, severely degrades regional water quality. During the 1990s fighting in Croatia, chemical manufacturing plants were bombed; because treatment facilities for chemical spills weren’t functioning, toxins flowed downstream unchecked until the conflict ended.
Increased Production
Even in regions not directly affected by warfare, increased production in manufacturing, agriculture, and other industries that support a war effort can wreak havoc on the natural environment. During World War I, former wilderness areas of the United States came under cultivation for wheat, cotton, and other crops, while vast stands of timber were clear-cut to meet wartime demand for wood products. Timber in Liberia, oil in Sudan, and diamonds in Sierra Leone are all exploited by military factions. “These provide a revenue stream that is used to buy weapons,” says Bruch.
Scorched Earth Practices, Hunting, and Poaching
The destruction of your own homeland is a time-honored, albeit tragic, wartime custom. The term “scorched earth” originally applied to the burning of crops and buildings that might feed and shelter the enemy, but it’s now applied to any environmentally destructive strategy. To thwart invading Japanese troops during the Second Sino-Japanese War (1937–1945), Chinese authorities dynamited a dike on the Yellow River, drowning thousands of Japanese soldiers—and thousands of Chinese peasants—while also flooding millions of square miles of land.
Biological, Chemical, and Nuclear Weapons
The production, testing, transport, and use of these advanced weapons is perhaps the single most destructive effects of war on the environment.8 Though their use has been strictly limited since the bombing of Japan by the U.S. military at the end of World War II,9 military analysts have grave concerns about the proliferation of nuclear material and chemical and biological weaponry.10 “We’ve been very fortunate that we have not seen the devastation that we might see,” says Bruch.
Researchers point to the use of depleted uranium (DU) as one particularly dangerous military trend.11 DU is a byproduct of the uranium-enrichment process. Almost twice as dense as lead,12 it’s valued in weapons for its ability to penetrate tank armor and other defenses. An estimated 320 tons of DU were used in the Gulf War in 1991; in addition to soil contamination, experts are concerned that soldiers and civilians may have been exposed to dangerous levels of the compound.13
How Environmental Problems Lead to War
While the effects of war on the environment may be obvious, what’s less clear are the ways that environmental damage itself leads to conflict. Factions in resource-poor countries like those in Africa, the Mideast, and Southeast Asia have historically used military force for material gain; they have few other options.
Bruch explains that once armed conflict begins, soldiers and populations under siege must find immediate sources of food, water, and shelter, so they’re forced to adapt their thinking to short-term solutions, not long-term sustainability.
This short-term desperation leads to a vicious cycle of conflict, followed by people who meet their immediate needs in unsustainable ways, bringing deprivation and disillusionment, which then leads to more conflict. “One of the chief challenges is to break that cycle,” Bruch says.
Can Warfare Protect Nature?
It seems counterintuitive, but some have argued that military conflicts often end up preserving the natural environment. “It’s one of the findings that’s utterly contrary to expectations,” says Jurgen Brauer, Ph.D., professor of economics at Augusta State University in Augusta, Georgia. “The most preserved area in all of Korea is the demilitarized zone because you have the exclusion of human activity,” he says.
Other researchers have noted that despite the massive amounts of herbicide use during the Vietnam War, more forests have been lost in that country since the war ended than during it, due to peacetime commerce and Vietnam’s quest for prosperity. The coal-black skies caused by the Kuwaiti oil fires in 1991 provided dramatic visual evidence of war-related environmental damage. However, these oil fires burned in one month roughly the amount of oil burned by the United States in a single day.
“Peace can be damaging, too,” says Dabelko. “You have some of these ironic twists.”
But experts are quick to emphasize that this is not an argument in favor of armed conflict. “War is not good for the environment,” adds Brauer, who is also an author of the book “War and Nature: The Environmental Consequences of War in a Globalized World.”
And Bruch notes that warfare only delays the environmental damage of peaceful human activity and commerce. “It may provide a respite, but the long-term effects of war aren’t that different from what happens under commercial development,” he says.
Winning the Peace
As military planning evolves, it becomes apparent that the environment now plays a greater role in successful combat, especially after an armed conflict ends. “At the end of the day, if you’re trying to occupy an area, you have a strong incentive not to ruin it,” Dabelko says. The aforementioned biblical quote from Deuteronomy about preserving trees is, perhaps, good advice for the ages.
And some warriors are learning that there’s more to be gained from preserving the environment than in destroying it. In war-torn Mozambique, former military combatants have been hired to work together as park rangers protecting the wildlife and natural habitats that they once sought to destroy.14
“That built bridges between the military and the park service. It has worked,” Bruch says. “Natural resources can be very important in providing jobs and opportunities in post-conflict societies.”
Long Covid-19 • Fever (83-99%) • Cough (59-82%) • Fatigue (44-70%) • Anorexia (20-84%) • SOB (31-40%) • Myalgia (11-35%) • Others: anosmia, loss of taste, GI, headache Who gets Long Covid-19? • Factors that appear to be associated with a greater risk of suffering from “Long COVID-19” appear to be: • Increasing age • Excess weight/ obesity • DM-2 ,COPD,CKD • Patients on immunosuppression medication ,organ transplant recipients • Multiple symptoms at presentation Fever • May be treated symptomatically with Paracetamol or non-steroidal antiinflammatory drugs. • Monitoring functional status in post-acute coivd-19 patients is not yet an exact science. Chest Pain Chest pain is common in post-acute covid-19 syndrome approximate incidence 12 to 44 %. The clinical priority is to separate musculoskeletal and other non-specific chest pain from serious cardiovascular conditions. Cardiopulmonary complications include myocarditis, pericarditis, myocardial infarction, dysrhythmias, and pulmonary embolus; they may present several weeks after acute covid-19. They are commoner in patients with pre-existing cardiovascular disease Cough • chronic cough as one that persists beyond eight weeks. Up to that time, and unless there are signs of super-infection or other complications such as painful pleural inflammation, cough seems to be best managed with simple breathing control exercises and medication where indicated. Thromboembolism • Covid-19 is an inflammatory and hypercoagulable state, with an increased risk of thromboembolic events. • Many hospitalized patients receive prophylactic anticoagulation. thromboprophylaxis. • If the patient has been diagnosed with a thrombotic episode, anticoagulation and further investigation and monitoring should follow standard guidelines. Neurological Sequelae • Ischemic stroke, seizures, encephalitis, and cranial neuropathies have been described after covid-19, but these all seem to be rare. • A patient suspected of these serious complications should be referred to a higher centre. • Common non-specific neurological symptoms, which seem to co-occur with fatigue and breathlessness, include headaches, dizziness, and cognitive blunting (“brain fog”). Breathlessness • A degree of breathlessness is common after acute covid-19. Severe breathlessness, which is rare in patients who were not Hospitalised,may require urgent referral. Breathlessness tends to improve with breathing exercises . • Pulse Oximeters may be extremely useful for assessing and monitoring respiratory symptoms after covid-19. • An exertional desaturation test should be performed as part of baseline assessment for patients whose resting pulse oximeter reading is 96% or above but whose symptoms suggest exertional desaturation (such as lightheadedness or severe breathlessness on exercise). • Typically, oxygen saturation (pulse oxymeter) would be a daily reading taken on a clean, warm finger without nail polish, after resting for 20 minutes; the device should be left to stabilize and the highest reading obtained should be recorded. Fatigue • The profound and prolonged nature of fatigue in some post-acute covid-19patients shares features with chronic fatigue syndrome described after otherserious infections including SARS, MERS, and community acquired pneumonia. • We found no published research evidence on the efficacy of eitherpharmacological or non-pharmacological interventions on fatigue after covid-19. • Patient resources on fatigue management and guidance for clinicians on returnto exercise and graded return to performance for athletes in covid-19 arecurrently all based on indirect evidence. Fatigue Management which may include: • Energy management – 3 P’s: plan, priorities and pace, • Anxiety- Re-assure normal for fatigue after viral infection • Routine Gentle activity within self assessed limitation Physical activity advice • Rest and Sleep • Hydration and nutrition • Pain
At the start of the coronavirus pandemic, doctors started to raise concerns around new cases of diabetes in people who had caught the virus.
Since early reports first came to light, we’ve seen results from larger studies looking at big groups of people who’ve recovered from coronavirus. One study tracked over 47,000 people in England who had been admitted to hospital because of coronavirus before August 2020. The researchers followed their health for up to seven months after they were discharged and found 5% of people went on to develop diabetes.
They also showed that people who’d been in hospital with coronavirus were 1.5 times more likely to be diagnosed with diabetes after they’d been discharged than people of the same age and background who hadn’t been in hospital with coronavirus.
In 2022, researchers in the United States published findings from their analysis of health insurance data from around 1.6 million children, under the age of 18 years.
They looked at who’d been diagnosed with diabetes between March 2020 – March 2021 and if there were any differences in rates of diagnoses between children who’d had coronavirus, children who hadn’t, and children who had other types of respiratory infections. The study didn’t distinguish between type 1 and type 2 diabetes.
The researchers studied two different sets of data. In both datasets, children who’d had coronavirus were more likely to later be diagnosed with diabetes than those who hadn’t had coronavirus or had a different type of respiratory infection.
In the first dataset, the researchers found after having coronavirus, children were around 2.5 times (166%) more likely to develop diabetes than children who hadn’t been infected. In the other dataset the increased risk was smaller, at 31%. These differences in risk are likely down to differences in the way data was classified and collected. Respiratory infections that weren’t coronavirus were not found to be linked with an increased risk of diabetes.
The evidence to suggest a link between coronavirus and new cases of diabetes is growing but there’s still a lot we don’t know. We can’t yet be sure if coronavirus is directly causing diabetes, or whether there are other factors that could explain the link.
What type of diabetes?
Small studies have suggested that rates of new type 1 diabetes diagnoses in children were higher in 2020 compared to average rates in previous years.
The causes of type 1 diabetes are complex, and scientists think that there are a variety of environmental and genetic reasons that could explain why the condition develops.
Viruses could be one of these reasons, but the evidence around this is mixed and we just don’t know for sure yet. And as coronavirus is so new, there’s a lot we still need to learn about how it interacts with our immune system and its longer-term effects.
Cases of new type 2 diabetes diagnoses have also been reported in people who have had coronavirus. This could be related to the effects of coronavirus on the body, or the effects of lifestyle changes due to the pandemic, speeding up a type 2 diabetes diagnosis or bringing existing type 2 to light.
Scientists are also looking into the possibility that coronavirus could be causing a new type of diabetes. Blood sugar levels in some people with coronavirus rise due to the stress the body is under when trying to fight the infection, or because of some of the drugs used to treat it. But we don’t yet know if, or when, high blood sugar levels in people with coronavirus return to normal after they have fully recovered.
What’s going on inside the body?
One theory is that inflammation inside the body caused by coronavirus brings about insulin resistance, a feature of type 2 diabetes, which means the body isn’t able to make proper use of the insulin it’s producing.
We also know that coronavirus uses a protein found on the surface of some cells, called ACE-2, to enter and infect them. ACE-2 is found in the pancreas and there’s some evidence that this makes it vulnerable to coronavirus infection.
Small studies looking at pancreas cells grown in the lab and pancreas samples taken from people who sadly died from coronavirus have suggested that the virus can enter and infect insulin-producing beta cells in the pancreas, causing them to die or change how they work. This means people can’t produce enough insulin.
Another theory suggests that when coronavirus infects the pancreas it could trigger the immune system to attack and destroy beta cells, a key feature of type 1 diabetes.
Research into the biological processes that explain how and why coronavirus could cause diabetes is at an early stage and we need to be cautious about applying what scientists see in the lab to what’s happening in people infected with the virus. And we need more research to look at the types of diabetes we’re seeing in people who have had coronavirus to understand whether these are cases of type 1 and type 2 diabetes or something new altogether.
Finding answers
Scientists are working hard to find answers and are building a database of new cases of diabetes in people with coronavirus, called the CoviDiab registry. This will give them the information they need to carry out more thorough studies and discover more.
On top of this, the government has pledged £18.5 million to fund research to better understand and treat the longer term effects of coronavirus. These projects could give us important insights into new cases of diabetes after coronavirus.
Research, including the PHOSP-COVID study, will also help us to fully understand if coronavirus can make existing type 2 diabetes worse in people who already live the condition. The UK-wide study is following 10,000 people who were in hospital with coronavirus to monitor the long-term impact of the virus on their health. This study will include people with type 2 diabetes and will help us to understand how their condition has been affected.
Essential (primary) hypertension occurs when you have abnormally high blood pressure that’s not the result of a medical condition. This form of high blood pressure is often due to obesity, family history and an unhealthy diet. The condition is reversible with medications and lifestyle changes.
OVERVIEW
What is primary hypertension?
Primary (essential) hypertension is high blood pressure that is multi-factorial and doesn’t have one distinct cause. It’s also known as idiopathic or essential hypertension. Above-normal blood pressure is typically anything over 120/80 mmHg. This means that the pressure inside your arteries is higher than it should be.
Why should I be concerned about essential hypertension?
Essential hypertension (now known as primary hypertension) damages your blood vessels. The condition worsens over time and can cause life-changing complications that include:
How is primary hypertension different from other forms of hypertension?
Other types of hypertension have one distinct cause. These include a medical condition or side effects of medications. When there is a direct cause, it’s known as secondary hypertension. Primary and secondary hypertension can co-exist, particularly when there’s an acute worsening of blood pressure control, a new secondary cause should be considered.
Conditions that can cause secondary hypertension include:
A diagnosis of primary hypertension is made when you have high blood pressure, but none of the conditions that cause secondary hypertension. The best way to know if you have it is by seeing a healthcare provider who will:
Review your medical history to rule out conditions that cause secondary hypertension.
Perform a blood pressure check to determine whether you have high blood pressure.
What happens during a blood pressure check?
Healthcare providers use a device with an inflatable arm cuff and dial. They inflate the cuff and watch the dial while listening to the force of blood through a stethoscope.
The test results in two readings:
Systolic pressure (top number) measures pressure when the arteries are full of blood.
Diastolic pressure (bottom number) measures pressure when the heart is at rest between beats.
Normal blood pressure is below 120/80 mmHg. If either number is higher, you may have hypertension. Your healthcare provider will take multiple readings at different time points before determining the next steps in your care.
Will I need any other tests?
If there are multiple high blood pressure readings, your healthcare provider may recommend 24-hour ambulatory blood pressure monitoring. This test regularly measures blood pressure over 24 hours, even while you sleep. Healthcare providers take the average of these readings to confirm or rule out a diagnosis of hypertension.
MANAGEMENT AND TREATMENT
What does primary hypertension treatment look like?
Primary hypertension treatment typically includes lifestyle changes and medications.
Various medications can lower your blood pressure, including:
Angiotensin-converting enzyme (ACE) inhibitors help the body produce less angiotensin, a protein that raises your blood pressure. Captopril tablets are one type of ACE inhibitor.
Angiotensin II receptor blockers (ARBs) are medications that prevent blood vessel narrowing.
Beta blockers slow your heart rate and reduce the heart’s output, which lowers blood pressure. Metoprolol extended-release capsules are one type of beta blocker.
Calcium channel blockers, like diltiazem tablets, decrease the amount of calcium in the blood vessels. This helps muscle tissue relax to relieve narrowing.
Diuretics, such as furosemide tablets, help the body eliminate excess water and sodium.
Vasodilators help muscles in blood vessel walls relax, making it easier for blood to flow through them.
PREVENTION
How can I prevent essential (primary) hypertension from worsening?
To prevent high blood pressure from worsening you can:
Follow all care instructions, such as taking medications in the precise dose at specific times each day.
Ask your healthcare provider whether other medications you are taking may affect your blood pressure.
Keep all follow-up appointments so your healthcare provider can determine whether treatments are meeting your needs.
Stick to lifestyle changes, like quitting smoking and eating healthy.
OUTLOOK / PROGNOSIS
What is the outlook for people with primary hypertension?
Many people lower their blood pressure with medications and lifestyle changes. Some people come off blood pressure medications after maintaining a healthy lifestyle. A small number of people experience no change in blood pressure despite trying several medications (resistant hypertension).
LIVING WITH
What’s important to know about living with primary hypertension?
Medications alone are not enough to lower your blood pressure. For the best results, you need to live a healthy lifestyle.
It can be challenging to change what you eat and break old habits. Some people benefit from the help of health coaches, therapists or trusted friends. Setting realistic goals can help you make steady progress and feel your best.
A note from Cleveland Clinic
Essential hypertension is high blood pressure that is not due to another medical condition. There can be many causes, including obesity, family history and an unhealthy diet. Even though the condition does not cause symptoms, it’s critical to manage it. Essential hypertension can lead to blood vessel damage, putting you at risk for life-threatening complications. With successful treatment, you can lower your blood pressure and preserve your health for years to come.
There are many health risks of chronic alcohol abuse, ranging from high blood pressure to stroke. People are most familiar with alcohol’s negative effects on the liver.
Heavy drinkers have an increased risk of jaundice, cirrhosis, liver failure, liver cancer, and many other conditions.
The definition of heavy drinking is consuming 8 drinks or more per week for women and 15 or more for men. Even a single binge-drinking episode can result in significant bodily impairment, damage, or death.
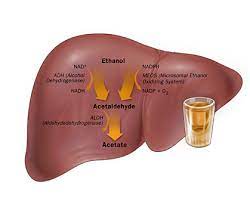
The liver breaks down and filters out harmful substances in the blood and manufactures the proteins, enzymes, and hormones the body uses to ward off infections. It also converts vitamins, nutrients, and medicines into substances that our bodies can use. The liver is also responsible for cleaning our blood, producing bile for digestion, and storing glycogen for energy.
The liver processes over 90% of consumed alcohol. The rest exits the body via urine, sweat, and breathing.
It takes the body approximately an hour to process 1 alcoholic beverage. This time frame increases with each drink. The higher someone’s blood alcohol content, the longer it takes to process alcohol. The liver can only process a certain amount of alcohol at a time. When someone has too much to drink, the alcohol left unprocessed by the liver circulates through the bloodstream. The alcohol in the blood starts affecting the heart and brain, which is how people become intoxicated. Chronic alcohol abuse causes destruction of liver cells, which results in scarring of the liver (cirrhosis), alcoholic hepatitis, and cellular mutation that may lead to liver cancer. These conditions usually progress from fatty liver to alcoholic hepatitis to cirrhosis, although heavy drinkers may develop alcoholic cirrhosis without first developing hepatitis.
Per University Health Network, a safe amount of alcohol depends on a person’s weight, size, and whether they are male or female. Women absorb more alcohol from each drink in comparison to males, so they are at greater risk of liver damage. Consuming 2 to 3 alcoholic drinks daily can harm one’s liver. Furthermore, binge drinking (drinking 4 or 5 drinks in a row) can also result in liver damage.
Mixing alcohol with other medications can also be very dangerous for your liver. Never take alcohol and medication simultaneously without speaking with your physician first. When combined, certain medications (such as Acetaminophen) can lead to severe damage to your liver. Other medications that are dangerous to combine with alcohol include Antibiotics, Antidepressants, Sedatives, and Painkillers.
Symptoms Of Liver Disease
Heavy drinkers face a higher risk of developing a range of liver diseases when compared to moderate drinkers. As many as 20% of heavy drinkers develop fatty liver disease, although fatty liver disease is typically reversible with abstinence. Alcoholic hepatitis, inflammation that causes liver degeneration, can further develop into cirrhosis and may even be fatal. However, this is also reversible with abstinence.
People who regularly abuse alcohol have a compounded risk of developing liver disease if they develop an infection or are genetically predisposed to liver problems. Those consuming more than 2 drinks on a daily basis put themselves at risk of liver disease.
Common symptoms of liver disease include:
Yellowish skin and eyes (jaundice)
Abdominal pain and swelling
Swelling in legs and ankles
Dark urine
Nausea or vomiting
Itchy skin
Discolored stool
Tendency to bruise easily
Chronic fatigue
Fever
Disorientation
Weakness
Loss of appetite
Pale, bloody, or tar-colored stool
Liver disease caused by alcohol is avoidable. Most reputable sources cite moderate alcohol consumption as 1 drink per day for women and 2 for men. In general, there isn’t a type of alcoholic beverage that is safer for the liver.
Treatment For Liver Disease And Alcoholism
Many forms of liver damage can be reversible if you stop drinking or take other steps.
Fatty Liver disease –Reversible with abstinence
Alcoholic Hepatitis –Reversible with abstinence
Cirrhosis –Abstinence is helpful; however, it is usually fatal due to secondary complications. These can include kidney failure or hypertension in the vein carrying blood to the liver. It could stabilize with abstinence but is case-by-case sensitive.
Liver Cancer –Same as cirrhosis
If you have an alcohol addiction and symptoms of liver damage, it’s important to find help as soon as possible.
Between 15% and 30% of heavy drinkers are diagnosed with cirrhosis each year, but the majority of those with this disease survive if they seek treatment for their addiction. Despite this, between 40% and 90% of the 26,000 annual cirrhosis deaths are alcohol-related.
Wind energy offers many advantages, which explains why it’s one of the fastest-growing energy sources in the world. Research efforts are aimed at addressing the challenges to greater use of wind energy. Read on to learn more about the benefits of wind power and some of the challenges it is working to overcome.
Advantages of Wind Power
Wind power is cost-effective. Land-based utility-scale wind is one of the lowest-priced energy sources available today, costing 1–2 cents per kilowatt-hour after the production tax credit. Because the electricity from wind farms is sold at a fixed price over a long period of time (e.g. 20+ years) and its fuel is free, wind energy mitigates the price uncertainty that fuel costs add to traditional sources of energy.
Wind creates jobs. The U.S. wind sector employs more than 100,000 workers, and wind turbine technician is one of the fastest growing American jobs. According to the Wind Vision Report, wind has the potential to support more than 600,000 jobs in manufacturing, installation, maintenance, and supporting services by 2050.
Wind enables U.S. industry growth and U.S. competitiveness. New wind projects account for annual investments of over $10 billion in the U.S. economy. The United States has a vast domestic resources and a highly-skilled workforce, and can compete globally in the clean energy economy.
It’s a clean fuel source. Wind energy doesn’t pollute the air like power plants that rely on combustion of fossil fuels, such as coal or natural gas, which emit particulate matter, nitrogen oxides, and sulfur dioxide—causing human health problems and economic damages. Wind turbines don’t produce atmospheric emissions that cause acid rain, smog, or greenhouse gases.
Wind is a domestic source of energy. The nation’s wind supply is abundant and inexhaustible. Over the past 10 years, U.S. wind power capacity has grown 15% per year, and wind is now the largest source of renewable power in the United States.
It’s sustainable. Wind is actually a form of solar energy. Winds are caused by the heating of the atmosphere by the sun, the rotation of the Earth, and the Earth’s surface irregularities. For as long as the sun shines and the wind blows, the energy produced can be harnessed to send power across the grid.
Wind turbines can be built on existing farms or ranches. This greatly benefits the economy in rural areas, where most of the best wind sites are found. Farmers and ranchers can continue to work the land because the wind turbines use only a fraction of the land. Wind power plant owners make rent payments to the farmer or rancher for the use of the land, providing landowners with additional income.
CHALLENGES OF WIND POWER
Wind power must still compete with conventional generation sources on a cost basis. Even though the cost of wind power has decreased dramatically in the past several decades, wind projects must be able to compete economically with the lowest-cost source of electricity, and some locations may not be windy enough to be cost competitive.
Good land-based wind sites are often located in remote locations, far from cities where the electricity is needed. Transmission lines must be built to bring the electricity from the wind farm to the city. However, building just a few already-proposed transmission lines could significantly reduce the costs of expanding wind energy.
Wind resource development might not be the most profitable use of the land. Land suitable for wind-turbine installation must compete with alternative uses for the land, which might be more highly valued than electricity generation.
Turbines might cause noise and aesthetic pollution. Although wind power plants have relatively little impact on the environment compared to conventional power plants, concern exists over the noise produced by the turbine blades and visual impacts to the landscape.
Wind plants can impact local wildlife.Birds have been killed by flying into spinning turbine blades. Most of these problems have been resolved or greatly reduced through technology development or by properly siting wind plants. Bats have also been killed by turbine blades, and research is ongoing to develop and improve solutions to reduce the impact of wind turbines on these species. Like all energy sources, wind projects can alter the habitat on which they are built, which may alter the suitability of that habitat for certain species.
One of the aspects of coronavirus disease 2019 (COVID-19) puzzling clinicians coping with management of the pneumonia that one of the disease’s complications is the presentation of patients with extremely low blood oxygenation, but no sensation of dyspnea [1]. This phenomenon has given rise to the term “happy hypoxemia” [1]. In the Wuhan cohort of patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-COV-2), only 19% complained of shortness of breath; 62% of those with severe disease and 46% of those who ended up intubated, ventilated or dead did not present with dyspnea [2]. What strikes us as odd, is that these patients are tachycardic with tachypnea and respiratory alkalosis. These signs suggest that at least some sensory information must reach the brainstem to elicit a partial compensatory reflex respiratory response that is sufficent to lower the CO2 level, which diffuses more rapidly across the alveoli than oxygen. However, these patients have no conscious awareness of hypoxia.
The homeostatic afferent information emanating from the body forms part of our interoceptive system, which senses the body’s physiological condition, creates awareness, and leads to conscious feelings or symptoms [3]. This process occurs via projections from the brainstem to the cortex that allow the brain to process homeostatic afferent signals. When the brain receives the signal of internal hypoxia, it gives rise to the sensation of “air hunger” and a need to breathe, which is curiously absent in severe COVID-19 patients.
The respiratory responses to hypoxia occur due to the presence of sensory nerves in chemoreceptive areas. These recognize the shift in the internal environment, relay the information to the brainstem, and stimulate an increase in the ventilatory drive. Respiratory pathology elicits autonomic reflexes, such as bronchospasm, secretions, or cough. Dyspnea is the conscious distressing symptom of difficulty in breathing that can be triggered by many clinical conditions [4]. In the setting of cardiopulmonary illness, dyspnea arises from inputs from multiple homeostatic afferents. Interoceptive processing of these signals create a sense of shortness of breath and the urge to breathe. This primitive brainstem reflex is essential for survival as it can respond to a wide range of stimuli, including hypoxia, hypercapnia, irritants, acidosis, airway collapse, and pulmonary vascular congestion.
The glossopharyngeal afferents innervating the carotid body, and the vagal afferents innervating the respiratory tract, play a vital role in monitoring organ function and controlling body homeostasis through activation of the autonomic nervous system. These neurons are the primary sensory inputs of a series of reflex circuits that control key visceral functions, including blood pressure, swallowing, gastrointestinal motility, airway caliber, and tidal volume [4]. They also produce the first afferents for the conscious sensation of dyspnea.
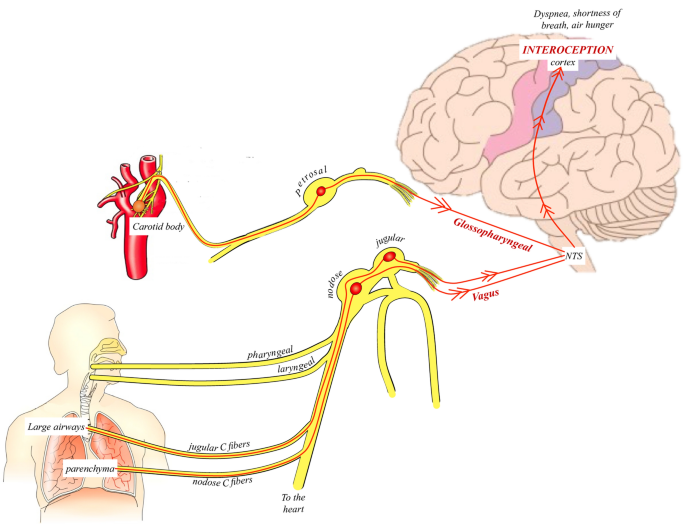
Mechanical or chemical stimuli of pulmonary receptors expressed on afferent vagal nerve terminals in the lung arrive in the brainstem through small-diameter myelinated (Aδ)- or unmyelinated (C)-fiber nerve axons with cell bodies in the jugular or nodose ganglia of the vagus (Fig. 1). Both jugular and nodose pulmonary C-fiber afferents respond to inflammatory mediators and tissue acidification in a graded fashion; these can be considered “nociceptive” fibers as they do not react to eupneic breathing or other regular events, but are excited by “noxious” or “potentially noxious” stimuli. The jugular and nodose nerve fibers of the lung have distinct differences in terms of their embryologic origin, pharmacological responses, and neurochemistry. Thus, they serve different functions–which are hard to tease apart in the intact human. The nodose C-fibers probably play a more prominent role in the genesis of dyspnea and the subjective sensation of breathing difficulty. In contrast, jugular fibers may play a more prominent role in coughing [4]. The vagal C-fiber afferents innervate the larynx response within seconds to laryngeal discomfort and appear to be important in stimulating cough. Meanwhile, the dyspneic sensation is specifically related to the activation of a subgroup of nodose vagal afferent that express adenosine receptors. The afferent information arriving from the vagal and glossopharyngeal nerves converges at the nucleus of the tractus solitarius in the medulla, a key relay site for a variety of other critical homeostatic signals. From here, there are connections to the higher centers of the brain towards the thalamus, somatosensory cortex, insular cortex, and amygdala, all involved in the perception of breathing.
Neurophysiology of dyspnea.
Neurophysiology of dyspnea. Main afferent (sensory) homeostatic information arising from areas of the vasculature and lungs give rise to the sensation of dyspnea. When stimulated, the chemoreceptive and mechanoreceptive signals are transmitted to the brainstem via the glossopharyngeal and vagus nerves, converging at the nucleus of the tractus solitarus (NTS). Subsequent projections continue to the somatosensory cortex and other higher brain regions, which provide the interoceptive sense of the internal environment of the body. The processing of these signals within the cortex gives rise to sensations such as air hunger, dyspnea, or shortness of breath. This interceptive processing appears to be abnormally blunted in patients with coronavirus disease 2019
The pathophysiology underlying the dissociation between profound hypoxemia and overt dyspnea in COVID-19 pneumonia is, at this point, unclear. In our experience, this disassociation exists in patients with severe lesions in the glossopharyngeal or vagus nerves due to damage to the cranial nerve after neck cancer or congenital neuropathies, but these findings are unexpectedly absent in the autopsy reports that are now emerging in COVID-19 cases.
The possibility that the novel SARS-COV-2 is neuro-invasive remains controversial. On one hand, in severe COVID-19 cases, neurological symptoms, such as anosmia, headache, altered mental status, seizures, and delirium, are common; and SARS-COV-2 is found in the cerebral spinal fluid and thought to enter the brain through synapse-connected routes [1]. The possible damage to the afferent hypoxia-sensing neurons in persons with COVID-19 could be due to the intense cytokine storm or the direct effect of SARS-COV2 on mitochondria or on the nerve fibers [1]. On the other hand, the findings from brain magnetic resonance imaging (MRI) studies and pathology reports in lethal COVID-19 cases are inconsistent and do not provide a pathophysiological correlate to explain the absence of dyspnea [5]. The common brain pathology findings in fatal COVID-19 cases are multiple areas of ischemic and micro-bleeding hemorrhagic strokes with only small regions of inflammation; however, it is worth noting that at least 40% of cases brain imaging studies were normal and there were no signals of brainstem abnormalities on the MRI scans. The neurological manifestations of other coronaviruses are even less well studied, but neuropathy and myopathy are reported in a handful of cases of both severe acute respiratory syndrome (SARS-CoV) and middle eastern respiratory syndrome (MERS-CoV). What makes COVID-19 most intriguing at this point is what the patient does not sense and what the brain does not show in terms of pathology.
Regardless of the uncertain underlying pathology, reduced perception of dyspnea is a disorder of blood-gas interoception. It may mask the severity of the medical status and ultimately delay patients from seeking urgent medical care. Patients admitted with COVID-19 can suffer sudden death after voluntary “breaks” from the oxygen supplementation. Recognizing “happy hypoxia” as a feature of COVID-19 pneumonia has led to better patient care, with physicians relying on other markers of disease, such as tachycardia, fever, or serum inflammatory acute reactants, to guide treatment or discharge patients from the hospital. Continuing research on how the novel coronavirus impacts peripheral sensors and neural pathways holds the promise of further clarifying its mechanisms.
UNEP executive director calls on UN member states to consider passing a resolution on right to a clean environment, on the lines of UN Human Rights Council
The United Nations Human Rights Council October 8, 2021, unanimously voted for recognising a clean, healthy and sustainable environment as a universal right in Geneva, Switzerland.
If recognised by all, the right would the first of its kind in more than 70 years since the Universal Declaration of Human Rights was adopted by the UN General Assembly in 1948.
Inger Anderson, the executive director of the United Nations Environment Programme (UNEP), hailed the development in a statement.
She also called on UN member states to consider a similar resolution at the General Assembly.
The right to a clean environment was rooted in the 1972 Stockholm Declaration, Anderson noted. It was greatly encouraging to see it formally recognised at the global level five decades later, she added.
Over 13,000 civil society organisations and indigenous peoples’ groups, more than 90,000 children worldwide, the Global Alliance of National Human Rights Institutions and private sector stakeholders had campaigned relentlessly for the right, Anderson said.
The resolution emphasises “the rights to life, liberty and security of human rights defenders working in environmental matters, referred to as environmental human rights defenders.”
Environmental defenders across the globe are subject to constant physical attacks, detentions, arrests, legal action and smear campaigns.
Some 200 environmental defenders have been murdered in 2020 alone. Anderson said the UNEP would deepen its commitment to protecting and promoting environmental human rights defenders in the coming months.
She added that her organisation expected the resolution to embolden governments, legislators, courts and citizen groups in pursuing substantial elements of the Common Agenda for renewed solidarity.
The Agenda was presented last month by UN Secretary-General Antonio Guterres. Anderson also called for these parties to pursue the 2020 Call to Action on Human Rights.
“Let no one be left behind, as we forge a healthier planet with less conflict and more space for youth to be heard,” she said.